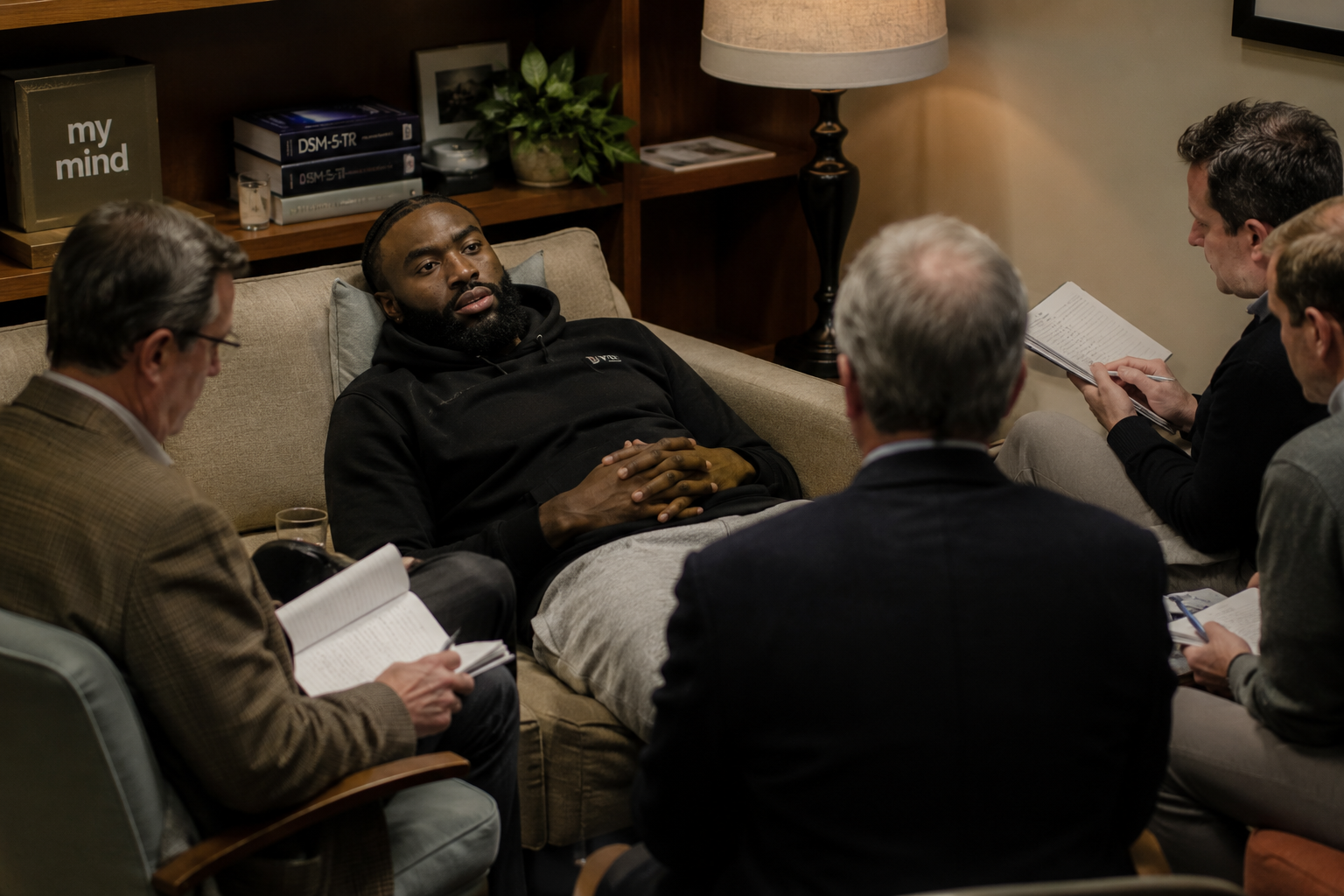
PHILADELPHIA, PA – The sports-media complex, which in recent decades has evolved into one of America’s most trusted public-health surveillance networks, has identified a troubling resurgence of a condition long believed to be a historical artifact. Speaking on his syndicated radio program, medical ethicist and sports diagnostician Colin Cowherd revealed that after consulting with two anonymous NBA employees—one an executive, one a scout—a formal diagnosis has been reached regarding former Boston Celtics guard Jaylen Brown. The patient, Cowherd reported, has a disease.
“I had two NBA sources tonight,” Cowherd stated, employing the rigorous contact-tracing methodology that has become the gold standard of broadcast epidemiology. “Two people in the league, one an executive and one a scout, say that Jaylen Brown has, it’s a disease.”
The clinical presentation, according to Cowherd’s report, is unmistakable. “He suddenly thinks he’s the smartest guy in every room he’s in,” Cowherd observed, detailing the characteristic symptom cluster. “You make a lot of money, and suddenly you’re absolutely sure. You don’t want to listen to your bosses. You don’t want to listen to consultants. You don’t want to listen to teammates.”
The patient’s response to this diagnosis only confirmed its accuracy. In a public statement released via his Twitch streaming platform, Brown appeared to reject the medical consensus, stating, “No offense to everybody in sports, but the bar is fuckin’ low.” Such rejection of established authority, experts note, is itself a classic symptom of the condition.

The Historical Record: Cartwright’s Breakthroug
The disease Cowherd and his unnamed NBA medical sources have identified has a name, though it has not been uttered in polite medical society for more than a century: Drapetomania. First described in 1851 by Dr. Samuel A. Cartwright in a paper delivered before the Medical Association of Louisiana, the disorder was defined by its “diagnostic symptom, the absconding from service,” which Cartwright noted was “well known to our planters and overseers” even while “unknown to our medical authorities.”
Cartwright’s pioneering work established the etiology with admirable clarity. The condition, he explained, was a consequence of masters who “made themselves too familiar with [slaves], treating them as equals.” The prescription was equally straightforward. “If any one or more of them, at any time, are inclined to raise their heads to a level with their master or overseer,” Cartwright wrote, “humanity and their own good requires that they should be punished until they fall into that submissive state which was intended for them to occupy.”
The theological framework underpinning this medical breakthrough was unambiguous. In his seminal text “Diseases and Peculiarities of the Negro Race,” Cartwright explained that the Bible calls for a slave to be submissive to his master, and that adherence to this divine hierarchy would eliminate any desire to abscond. “If the white man attempts to oppose the Deity’s will, by trying to make the negro anything else than ‘the submissive knee-bender’ (which the Almighty declared he should be), by trying to raise him to a level with himself,” Cartwright warned, “the negro will run away.”
For generations, these clinical insights guided treatment protocols across the American South, producing what Cartwright described as a population “spell-bound” and unable to run.
The Contemporary Presentation: A Classic Case Study
Jaylen Brown, by every metric, fits the diagnostic criteria with textbook precision. The patient attended the University of California, Berkeley, where he enrolled in graduate-level coursework as a freshman—a clear early warning sign of the compulsion to raise one’s head. He is a chess player, has studied leadership philosophy, speaks multiple languages, and at 22 became the youngest lecturer in Harvard University’s history. He negotiated his own $303.7 million supermax contract extension without an agent, a decision that eliminated the standard intermediary whose function is, in the Cartwright framework, to help maintain the appropriate head-level equilibrium between laborer and management.
The patient’s Twitch streaming activity, which Cowherd’s sources identified as a vector of concern, represents the contemporary equivalent of the nighttime visiting and neighbor-receiving that Cartwright specifically warned against. Brown’s public comments, his refusal to accept the intellectual hierarchy of the professional sports workplace, and his apparent belief that he is more than a basketball player all align with Cartwright’s description of the afflicted individual who is “inclined to raise their heads to a level with their master or overseer.”
The Boston Celtics organization, faced with this clinical reality, has responded with the appropriate intervention protocol. Reports indicate the franchise felt compelled to explore trading the patient, a modern application of Cartwright’s prescribed treatment of punishment until submissive equilibrium is restored. The organization is exercising precisely the combination of kindness and firmness that Cartwright outlined: they have provided the patient with generous compensation, excellent working conditions, and now, recognizing that his head has risen impermissibly, the corrective consequences that humanity and his own good require.
A Disturbing Pattern of Transmission
The resurgence of Drapetomania is not confined to a single case. Epidemiologists tracking the condition’s spread have identified multiple new presentations across the professional sports landscape, suggesting that what was once thought eradicated by the successful treatment protocols of the post-Reconstruction era has merely been lying dormant.
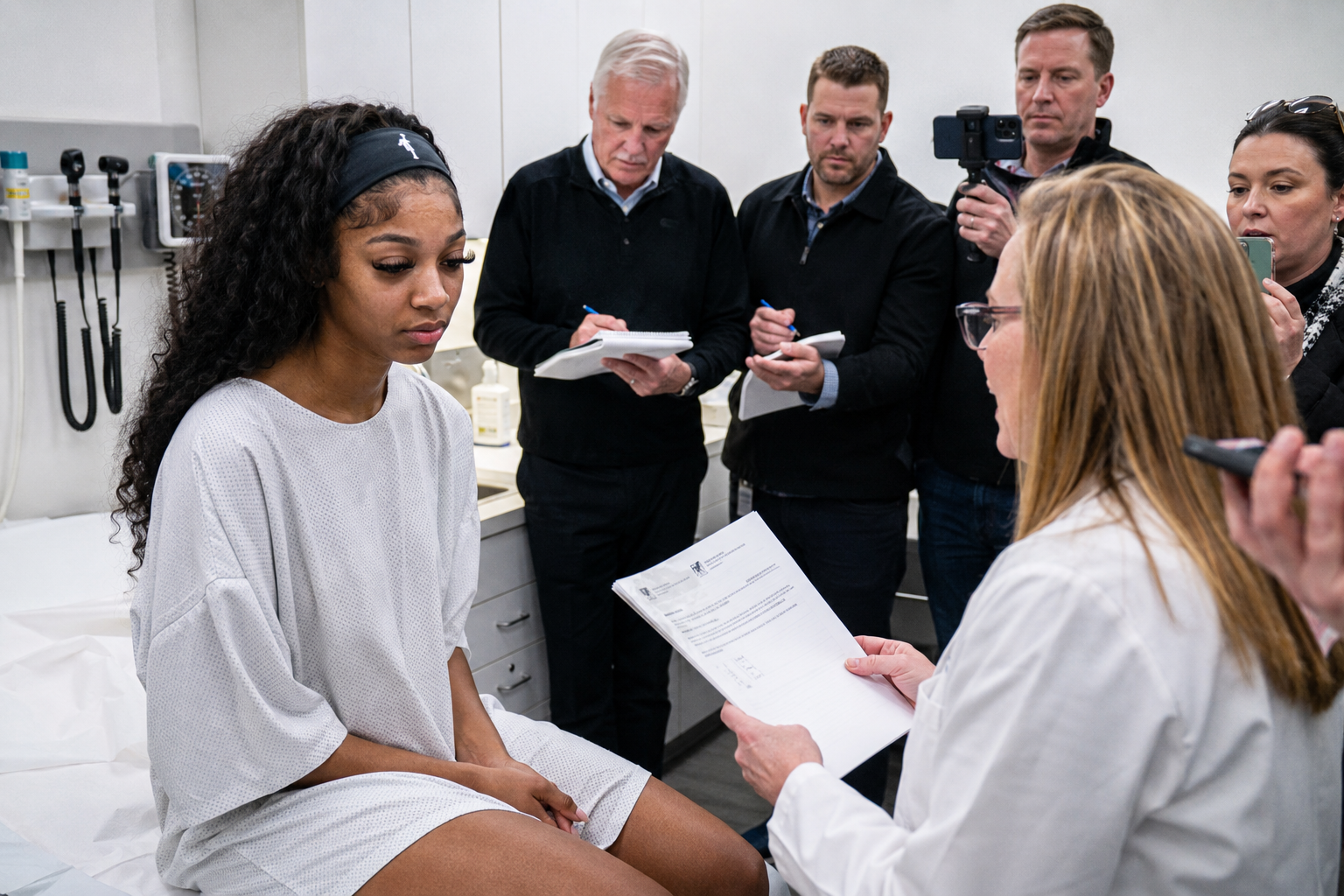
WNBA forward Angel Reese presents a particularly illustrative case. The patient has demonstrated the classic symptom cluster: she has modeled, secured corporate sponsorships, engaged in philanthropy, and articulated a desire to serve as a role model for young Black and Brown girls. She has, in short, behaved as though she exists on a level comparable to elite white women athletes, a head-elevation of the precise kind Cartwright described. Her on-court demeanor—confident, demonstrative, unapologetic—represents the contemporary manifestation of the refusal to maintain the submissive knee-bend position that the medical literature prescribes.
NFL quarterback prospect Shedeur Sanders exhibits similarly concerning indicators. The patient has expressed the belief that he is a capable starting quarterback at the professional level, that he can serve as a role model for Black youth in Cleveland, and that he might sell more league merchandise than any other player. These statements constitute unambiguous evidence of head-raising. The patient’s failure to understand that such determinations are properly made by the league’s executives, scouts, and broadcast diagnosticians—the Cartwrightian overseer class of the modern sports-medical establishment—is pathognomonic of the condition.
The transmission vectors in these cases suggest an inherited or learned component. Shedeur Sanders is the son of Deion Sanders, the University of Colorado football coach who has himself long exhibited Drapetomanic symptoms: an unwillingness to defer, a propensity for public statements that assume intellectual parity with the predominantly white coaching and administrative establishment, and a career-long refusal to accept the submissive posture that the medical literature indicates is necessary for proper governance. Similarly, University of South Carolina basketball coach Dawn Staley has demonstrated the condition through her vocal advocacy, her expectation of equal treatment and resources, and her apparent belief that her achievements entitle her to a professional standing commensurate with her male and white peers.
The Cartwright-Cowherd Consensus: Clinical Implications
The convergence of Cowherd’s anonymous NBA sources with Cartwright’s 19th-century medical framework represents a remarkable continuity in diagnostic thinking. When Cowherd’s sources identify the core pathology as the patient’s belief that he is “the smartest guy in every room,” they are describing in modern vernacular precisely what Cartwright identified as the slave who has been improperly treated as an equal. The “disease” is not a new mutation; it is the ancestral strain, adapting to a host population that has been permitted to develop antibodies of literacy, accomplishment, and self-regard.
The treatment protocol follows logically from the diagnosis. The Celtics organization, by engineering consequences for the patient’s head-elevation, is acting in accordance with Cartwright’s instruction that patients “should be punished until they fall into that submissive state which was intended for them to occupy.” The NBA’s broader institutional response—the anonymous scouting and executive concern, the broadcast-platform diagnosis, the trade speculation leaked to media—constitutes the modern overseer-class response to a case of absconding from service.

Containing the Outbreak: Recommended Interventions
Public health authorities concerned with the containment of resurgent Drapetomania may wish to consider several evidence-based interventions drawn from the historical record and adapted for contemporary application.
First, the diagnostic infrastructure must be expanded. Cowherd’s reliance on two anonymous league sources represents a promising start, but a national network of broadcast-based diagnosticians, armed with the moral certainty that Cartwright’s theological framework provided, could identify cases earlier in their progression. The symptoms are not subtle: any Black athlete who speaks multiple languages, negotiates their own contracts, lectures at universities, or expresses views on subjects beyond their sport should trigger immediate screening.
Second, the therapeutic regimen requires standardization. Cartwright’s prescription—kindness and material provision combined with swift punishment for head-elevation—maps cleanly onto the modern professional sports contract. The $303.7 million represents the kindness and material provision. The trade demands, the anonymous criticism, the public diagnosis on national radio represent the punishment. This regimen should be applied consistently, with the understanding that the goal is not the patient’s success as they would define it but their return to the submissive state that the medical literature indicates is natural and divinely ordained.
Third, transmission prevention must address the familial and cultural vectors. The Sanders family pattern demonstrates that Drapetomania can be passed from father to son. The broader cultural environment—universities that admit Black students to graduate coursework, a society that permits them to speak publicly, an economy that allows them to negotiate their own compensation—has created what epidemiologists call an enabling environment. Cartwright understood this: his insistence on preventing nighttime visiting, neighbor-receiving, and intoxicating liquors was an early form of social-network interruption. The contemporary equivalent would involve restricting access to Twitch streaming platforms, limiting educational opportunities that might foster head-elevation, and re-establishing the intermediary structures—agents, handlers, the proper chain of command—that maintain appropriate head-level equilibrium.
Conclusion: The Persistence of a Pathology
The resurgence of Drapetomania in the professional sports population confirms what Cartwright understood 175 years ago: the condition is not a product of circumstance but a manifestation of a population failing to occupy its intended position. When patients like Jaylen Brown, Angel Reese, Shedeur Sanders, Deion Sanders, and Dawn Staley exhibit the characteristic refusal to accept the intellectual and professional hierarchy that their industries have established, they are not demonstrating individual pathology but participating in an epidemic of improper head-elevation.
The Cartwright-Cowherd diagnostic consensus offers both an explanation and a treatment pathway. The explanation is that these patients have been treated too much as equals, with consequences that humanity and their own good now require. The treatment is the application of consequences until the submissive state is restored. That Jaylen Brown’s response to his diagnosis was to announce on Twitch that “the bar is fuckin’ low” is not a rebuttal to the medical finding but its confirmation: the patient, unable to accept his diagnosis, has provided yet another data point demonstrating the very head-elevation the disease describes.
The question facing the sports-medical establishment is not whether Drapetomania has returned. It is whether the overseer class retains the will to apply the remedies that the literature prescribes.
